Steps 3 and 4 of the logical framework approach provided in the figure for introducing or reviewing a CSE programme could be done through a situation analysis and/or a landscape analysis.
A situation analysis is a systematic method for reviewing the overall context, health status, and well-being of adolescents in a country or sub-region. It uses available data to identify the adolescents facing the greatest need for CSE, sexual and reproductive health services and other programmes. A CSE situation analysis should examine:
- The main issues affecting adolescents and the contexts in which they take place
- Harmful practices affecting adolescents (e.g., levels of child marriage, FGM/C, IPV, etc.)
- The socio-cultural context of their lives, including the protective and risk factors at various levels (e.g., individual, family, peer, community, etc.) and with institutions (e.g., schools, health services, employment, etc.) that can influence their health
- The co-morbid conditions and behaviours that can have an impact on sexual and reproductive health (e.g., HIV status, use of alcohol and/or drugs, etc.).
(Adapted from: Every Woman Every Child, 2017: “Technical Guidance for Prioritizing Adolescent Health”)
A landscape analysis should:
-
identify and map existing programmes, policies, and projects that address adolescent issues in general by geographic area, the socio-demographic characteristics of the beneficiaries, as well as the results and outcomes from these programmes.
-
identify the stakeholders and organisations involved in planning, managing, implementing, monitoring and evaluating these activities, at the national and sub-national level.
-
identify the systems that are in place to support capacity development, supportive supervision, coordination, and other planning and management functions. Crucially, it should examine how adolescents and youth participate in and contribute to these efforts, and the systems or platforms in place for them to do so.
-
seek to identify existing and potential sources of financing (domestic and international) and current budgetary allocations, especially how they meet the required needs.
(Source: Every Woman Every Child, 2017: “Technical Guidance for Prioritizing Adolescent Health”)
When designing a CSE intervention at the community or school level, it is important to consider three questions:
-
What is the community’s need?
-
How ready is the community to implement CSE?
-
What are the goals and objectives of the CSE implementation?
Question One: What is the Community’s Need?
Individual communities need different types of CSE programming, and will be able to implement them at varying levels and extents. The two best ways to determine a community’s needs is by using available data and/or conducting a needs assessment.
Relevant country-level data is usually maintained by ministries of health, education or statistics and can also be found on the Demographic and Health Surveys (DHS) site. Community-level data can often also be found through ministries of health, or other local governmental entities and departments of health.
Conducting a needs assessment can help communities to:
• Clearly determine both the met and unmet CSE needs within a specific area.
• Identify target populations’ needs in addition to the general population (e.g., girls, LGBTQI+ youth, etc.).
• Define the program’s purpose and scope.
• Develop appropriate goals and objectives, and corresponding program interventions and activities.
• Establish a baseline from which to measure program achievements over time.
• Further elicit community support for the program.
• Collect data to meet funder requirements and to seek additional funding.
(Source: CDC (2014) – “Practical Use of Program Evaluation Among STD Programs: Describe the Program”
“Practical Use of Program Evaluation Among STD Programs:
There are numerous methods for conducting a needs assessment. This table offers some of the most common methods, with their accompanying intentions and uses:
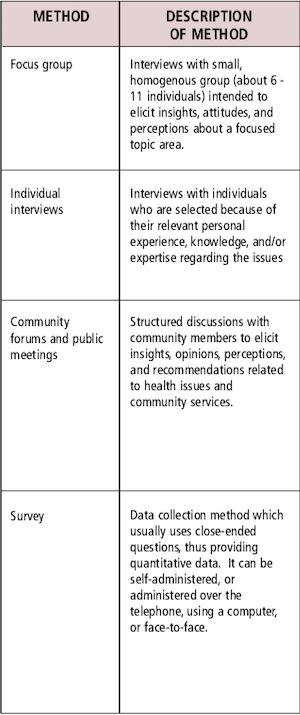
(Source: CDC, 2014 – “Practical Use of Program Evaluation Among STD Programs: Describe the Program”
“Practical Use of Program Evaluation Among STD Programs:
Question Two: How ready is the community to implement CSE?
Readiness levels for CSE can increase and decrease. The amount of time it takes to move to a higher readiness level can vary by the topic, by the intensity and appropriateness of community efforts, and by external events (such as an incident that puts focus on the issue, such as an increase in teen pregnancy or a sexual assault in a community).
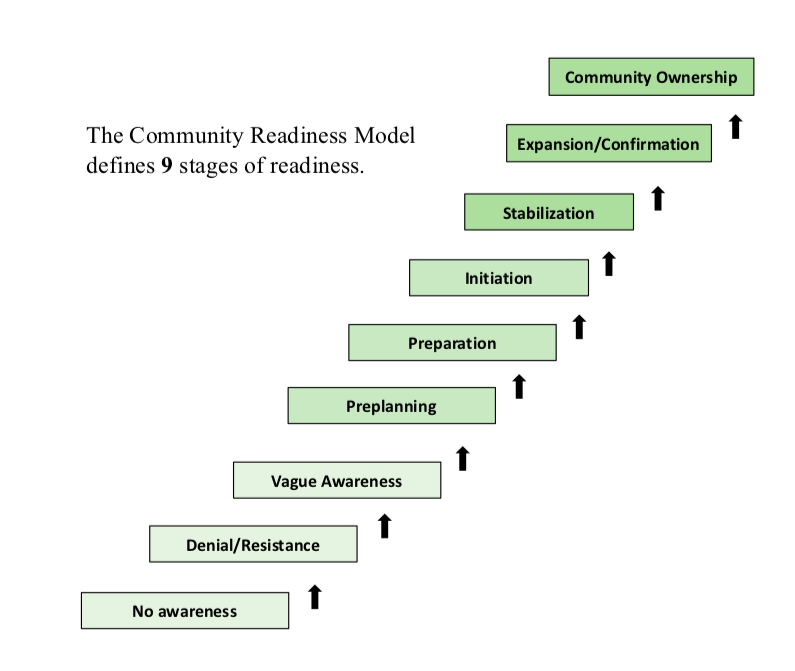
Given this variability in readiness, it can be useful to contextualize a community’s readiness by stages. Understanding the stage a community’s leadership and members are in provides valuable information to support programme design, management and sustainability.
Stage 1: No Awareness
• Leadership believes CSE is not important.
• The community believes there are more important topics to focus on other than CSE.
• Community members have no knowledge about what CSE is and how it supports the overall health and well-being of young people.
Stage 2: Denial/Resistance
• Leadership and community members do not believe young people in their community need sexuality-related information, or think it is inappropriate to provide it.
• Only a few community members have knowledge about CSE, and there are misconceptions among community members about CSE.
Stage 3: Vague Awareness
• Leadership and community members believe that CSE may be important to a community, but show no immediate intention to act.
• Leadership and community members may agree that something should be done to address young people’s need for sexuality information, but do not know what to do.
Stage 4: Preplanning
• Leadership and community members are open to partnering with outside CSE experts to create a plan of action.
• Community members acknowledge the importance of CSE and are open to hearing about and playing a role in an intervention.
Stage 5: Preparation
• Leadership and community members are actively supportive of continuing or improving efforts to provide CSE
• Plans are put into place to move forward, such as funding, programme parameters, timing and more.
Stage 6: Initiation
• Programming begins. The leadership and community feel a sense of connection and responsibility toward the programme, and will be involved in the programme.
Stage 7: Stabilization
• Leadership is actively involved in the long-term sustainability of CSE efforts.
• The attitude in the community is “We have taken responsibility”. There is ongoing community involvement in supporting and delivering CSE.
Stage 8: Confirmation/Expansion
• Leadership plays a key role in expanding and improving efforts, including, but not limited to, scale-up efforts.
• The majority of the community strongly supports CSE efforts. Youth participation and donor and family investment in the programme is high.
Stage 9: High Level of Community Ownership
• Leadership is continually reviewing evaluation results of the efforts and is modifying financial support accordingly.
• Most major segments of the community are highly supportive and actively involved.
• Community members see CSE as an important part of the fabric of the community.
As with behaviour change models, the use of a community readiness staging model helps programmers confirm where a community is currently around CSE implementation, while also providing a road map to where they hope to bring a community by the conclusion of implementation. Although it is ideal to bring a community through all 9 stages, achieving stage 7 should also be considered a success.
Source: Cornell University ACT for Youth Center for Community Action (2020) – “CAPP Community Readiness”)
-
Question Three: What Are the Goals and Objectives of the CSE Implementation?
There are numerous ways to set goals for a programme. Many institutions or organisations find setting SMART goals to be most useful. SMART goals or objectives are those that are:
Specific – focusing on the who/what/when and where of what you want to achieve
Measurable – what you do should be able to be measured, counted or observed
Achievable – your goal should be realistic and achievable
Relevant – the change you aim to make should be based on an identified need, suited to your context
Time-bound – the time-frame for achieving your goals and objectives should be realistic.
(Source: UNESCO, IPPF and The PACT – 2017: “We Demand More! A Sexuality Education Advocacy Handbook for Young People”)
Objectives are different from goal statements in that they are concrete statements describing how a programme will reach their goals. They are more short-term, specific and outcome-based. Objectives can be assessed at the conclusion of a programme to see whether they were achieved and therefore the initiative successful.
Objectives identify:
- Who will be reached (target audience)
- What change will be achieved (e.g., increase in number of young people receiving CSE)
- In what time period the change will be achieved (e.g., over a six-month period)
- Where the programme will take place (e.g., in school-based settings).
(Source: The Partnership for Maternal, Newborn and Child Health and Women Deliver, 2018 – Advocating for Change for Adolescents!)